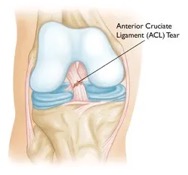
ACL Injury and Re-Injury Risk: What to Watch Out For
ACL tears are one of the most common injuries among adolescent athletes.3 Even with successful ACL replacement surgeries, some athletes still tend to re-injure themselves with another ACL injury.3 What makes some people more prone to this injury over others? Is it just bad luck or is there more to it? Due to the prevalence of this injury, the risk factors for ACL injury have been studied extensively. While this is a very complex question, let’s focus on one well researched risk area: biomechanics.
Biomechanical Risk Factors
Biomechanics are the ways in which our joints and muscles work together to move the body. Looking at biomechanics can be a good way to assess someone’s risk of ACL injury. Some of the more abnormal or risky movements can be spotted just through trained observation. ACL injury studies often look at biomechanics of landing, since this is often when ACL injuries occur and it can highlight any weak areas. The following biomechanical habits may lead to higher risk of ACL injury.1,2,3
- Increased hip flexion during landing:1,2 Athletes who tended to land more bent forward at the hip were more likely to suffer an ACL tear at some point.
- Increased internal hip rotation during landing:2 Some athletes tended to have their hip on the uninjured leg collapse in toward their body during landing. If this is the case, the risk of injury increases by a factor of 8.
- Knee valgus in female athletes:1,2 Female athletes who landed with increased knee valgus, knees falling into a “knock-kneed” position, were 3.5 times more likely to suffer an ACL injury compared to those who were not injured. This is more commonly seen in females rather than males.
- Decreased knee flexion during landing:1,2 knee bend during landing allows for a “softer” landing, giving your legs more time to absorb the forces of landing. If someone lands with a stiffer, more upright landing, they are more at risk of injury. One study found those who landed with less than 20° knee flexion were more likely to tear their ACL2EDIT.
- Side-to-side differences between the legs:2,3 Differences in strength, landing biomechanics, and single leg stability between each leg were all found to put an athlete at more risk. The typical goal is to achieve at least 90% equal leg strength between the non-injured leg and injured leg before athletes return to sports. For example, if you can push 100 lbs of weight with the uninjured leg, you would need to be able to push at least 90 lbs of weight with the injured leg.
- Decreased range of motion in the ankle:1 Those who landed in a more flat-footed position without the ability to bend at the ankle were more likely to suffer an ACL injury.

How PT Can Help
So, if you are exhibiting any of these characteristics when landing, how likely are you to injure or re-injure your ACL? There is no way to predict this with 100% accuracy, but looking for these biomechanical risk factors is a good start. The more abnormal landing habits/asymmetries that are present, the higher the risk of sustaining an ACL injury. Your physical therapist can help identify these habits, determine what might be causing them, and address any deficits. Through strengthening, motor control training, and sport-specific rehab, these habits can be improved upon to help athletes return to their sport safely and confidently! Schedule an appointment with one of MTI Physical Therapy’s highly trained physical therapists and get started today.
Sources
- Larwa, J.; Stoy, C.; Chafetz,R.S.; Boniello, M.; Franklin, C. Stiff Landings, Core Stability, and Dynamic Knee Valgus: A Systematic Review on Documented Anterior Cruciate Ligament Ruptures in Male and Female Athletes. Int. J. Environ. Res. Public Health 2021, 18, 3826. https://doi.org/10.3390/ijerph18073826
- Paterno, M. V., Schmitt, L. C., Ford, K. R., Rauh, M. J., Myer, G. D., Huang, B., & Hewett, T. E. (2010). Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. The American journal of sports medicine, 38(10), 1968–1978. https://doi.org/10.1177/0363546510376053